Why Watchful Waiting Fails Scoliosis Patients and What the Research Actually Says
By Dr. Justin M. Dick, DC — Founder, Clear Life Scoliosis and Chiropractic Center | CLEAR Scoliosis Institute Fellow and Board Member | ISICO World Master | PubMed-Indexed Researcher
Scoliosis affects an estimated seven million Americans. Most of them will be told the same thing after diagnosis: watch and wait. For curves below 25 degrees the standard recommendation is observation at four to six month intervals with no active intervention. This approach is presented to families as conservative and safe. It is neither.
Watchful waiting is a passive protocol applied to an active condition. Adolescent idiopathic scoliosis does not pause between appointments. In skeletally immature patients curves can progress rapidly during growth spurts. The window for non-surgical intervention narrows with every degree of progression and every month of skeletal maturation. Waiting is not neutral. It has a biological cost.
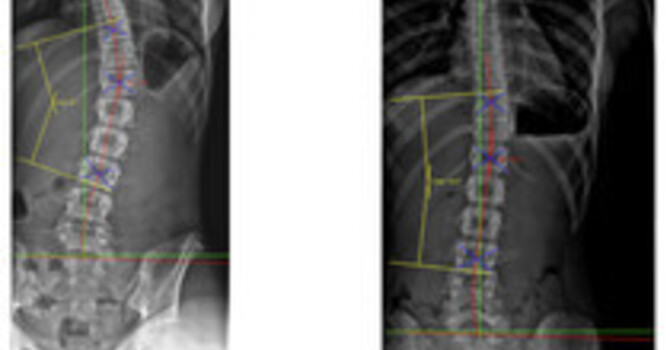
The clinical literature supports early intervention in ways that most families never hear about. Research published through the CLEAR Scoliosis Institute demonstrates that multimodal conservative treatment including scoliosis-specific exercise, corrective bracing, and structural chiropractic rehabilitation can reduce Cobb angle measurements and slow, halt, and the ability to reduce curves in patients. These are not anecdotal outcomes. They are documented in peer-reviewed literature with radiographic measurement as the outcome standard.
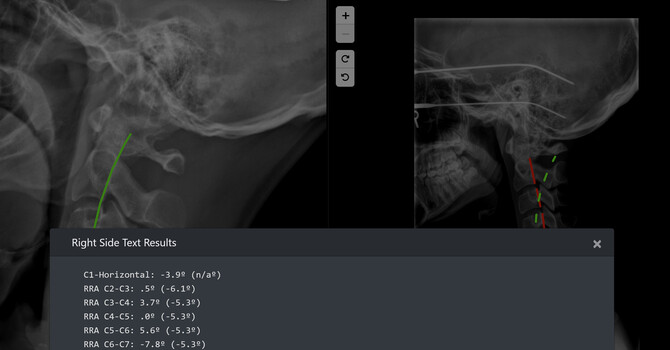
I have published seven papers in indexed medical journals examining scoliosis biomechanics, cervical sagittal alignment, and kinetic chain alterations in scoliosis patients. One consistent finding across this published body of work is that the structural consequences of scoliosis extend well beyond the primary curve. Geriatric patients present with decades of compensatory loading patterns that originate from curves that were observed rather than treated during their developmental years. The pain and disability these patients carry in their sixties and seventies is not simply aging. It is the compounded result of unaddressed structural imbalance.
The watchful waiting protocol also fails patients psychologically. A parent bringing a thirteen year old daughter to an orthopedic appointment after a school screening leaves with a diagnosis and no treatment plan. The family goes home and waits. They search online. They find forums filled with accounts of rapid progression and surgical outcomes. Anxiety fills the clinical void that the observation protocol creates. In my practice at Clear Life Scoliosis and Chiropractic Center I replaced the phrase watch and wait with monitor and measure years ago. The distinction matters. Monitoring implies active surveillance with defined thresholds. Waiting implies passivity. Families respond differently to each framing and compliance with home exercise and follow up care improves when the plan feels purposeful rather than passive.
The surgical threshold deserves scrutiny as well. Curves above 45 to 50 degrees are typically referred for surgical consultation and spinal fusion remains the dominant intervention at that stage. Fusion achieves curve correction but it also permanently alters spinal biomechanics. Motion is lost at fused segments. Adjacent segment degeneration is a well-documented long-term consequence. Patients who undergo fusion in adolescence carry the biomechanical consequences of that surgery for decades. Non-surgical intervention that prevents a curve from reaching surgical threshold is not just a conservative choice. It is a fundamentally different long-term outcome.
The research community has made meaningful progress on conservative scoliosis care in the past decade. Bracing evidence has strengthened considerably since the BrAIST trial demonstrated that bracing reduces the rate of curve progression to surgical threshold in skeletally immature patients. ScoliBrace and other three-dimensional corrective bracing systems have advanced well beyond the rigid TLSO designs that characterized earlier bracing protocols. Scoliosis-specific exercise approaches developed through ISICO have accumulated a growing evidence base. These tools exist. They work in appropriately selected patients. They are not yet reaching the majority of families who need them because the watchful waiting protocol remains the default recommendation at the point of diagnosis.
Clinicians managing scoliosis patients owe them more than a monitoring schedule. They deserve an honest conversation about what conservative intervention can realistically accomplish at their specific curve magnitude and skeletal maturity. They deserve defined thresholds that move the plan from observation to action. They deserve access to research that exists outside the surgical corridor.
Watchful waiting protects clinicians from overtreatment concerns. It does not protect patients from progression. These are not the same thing and the distinction should matter more than it currently does in clinical practice.
Justin Dick
Contact Me