When a patient or parent asks how fast scoliosis progresses, the honest answer is: it depends on variables that need to be measured, not estimated. Progression rate is not a fixed biological property of the condition. It is a function of the patient's skeletal maturity, the curve's location in the spine, the rate of growth occurring at the time of measurement, and whether degenerative changes are active. Each of those variables is assessable. None of them should be guessed.
The clinical problem is that "watch and wait" — the standard recommendation for mild scoliosis in growing patients — treats progression risk as if it is low and uniform across the population. It is neither. At Clear Life Scoliosis and Chiropractic Center in Charlotte, NC, the initial evaluation establishes the specific progression risk profile for each patient before a treatment plan is built. Dr. Justin M. Dick, DC — CLEAR Fellow, Board of Directors, multiple PubMed-indexed publications — evaluates Risser stage, curve location, growth velocity, and degeneration status as the foundation of every treatment decision. No referral required. Call 980-368-0766.
Schedule Your Evaluation Call 980-368-0766
What Drives Scoliosis Progression — The Four Variables That Actually Matter
1. Skeletal Maturity — Risser Stage
The Risser sign — the degree of ossification of the iliac apophysis visible on a standing AP radiograph — is the most clinically useful single marker of remaining skeletal growth. It is graded 0 through 5: Risser 0 indicates no ossification and significant remaining growth potential; Risser 5 indicates complete fusion and skeletal maturity. A patient at Risser 0 with a 20-degree thoracic curve is in a fundamentally different clinical situation from a Risser 4 patient with the same curve — the treatment urgency, progression risk, and expected curve behavior are categorically different.
The Risser stage does not tell the whole story. Two patients at Risser 1 can have very different growth velocities depending on where they are in the pubertal sequence. Girls who have not yet reached menarche are at higher progression risk than girls who have, even at the same Risser grade. Skeletal maturity assessment is more accurate when Risser stage is combined with pubertal staging and, where available, bone age imaging.
2. Growth Velocity and Pubertal Timing
Growth is the primary driver of scoliosis progression in adolescents. The relationship is mechanical — as the vertebral column lengthens rapidly during a growth spurt, the rotational and lateral components of an existing curve are amplified. The pubescent growth spurt is characterized by rapid and unpredictable velocity changes, which is precisely why "watch and wait" carries real clinical risk in a Risser 0 or Risser 1 patient with an existing structural curve.
The conventional argument for watchful waiting — that mild curves may not progress significantly — understates the risk created by the interval between monitoring appointments. A patient seen every six months during an active growth spurt can progress 8 to 12 degrees in that interval. That is the difference between a 20-degree curve requiring close monitoring and a 30-degree curve approaching the bracing threshold. The monitoring interval itself is a clinical decision, not an administrative convenience.
Adolescent idiopathic scoliosis — the most prevalent type overall — is diagnosed between ages 10 and 18 and represents the highest-risk population for rapid progression precisely because they are entering or actively in the fastest growth phase of their lives. See About Scoliosis for the full clinical picture of AIS.
3. Curve Location
Not all curve locations progress at the same rate. Thoracic curves — the most common location — are also the most prone to rapid progression. The mechanical reason is that the thoracic spine attaches to the rib cage, which means the rotational component of a thoracic curve produces rib cage deformation that amplifies as the curve increases. The thoracic spine is also less inherently stable than the lumbar spine, which contributes to faster progression during growth spurts.
In older adults, the lumbar spine becomes the location most vulnerable to rapid progression. The lumbar vertebrae bear the compressive load of the entire spinal column above — torso weight, thoracic and cervical spine, head — in addition to the forces of movement and activity. As degenerative changes accumulate in the lumbar discs and facet joints, asymmetric loading accelerates curve progression at a rate that exceeds what the same patient would have experienced during adolescence.
4. Degeneration Status
The assumption that scoliosis stabilizes at skeletal maturity is not supported by longitudinal data. Adult idiopathic scoliosis — most often pre-existing adolescent curves that become symptomatic in adulthood as compression begins — progresses at approximately 0.5 to 1 degree per year without intervention. Over a decade, that is 5 to 10 degrees of additional curve magnitude. Over two decades, it can push a previously manageable curve toward surgical consideration.
When the degenerative cycle is active, progression accelerates significantly. Degenerative scoliosis — driven by asymmetric disc height loss, facet joint arthropathy, and vertebral endplate changes — can progress at 4 degrees per year. That rate is clinically significant. A patient who presents at 35 degrees and is told to monitor without intervention can reach the surgical threshold of 50 degrees within five years if degenerative progression is active.
The initiating factors for the degenerative cycle include chronic postural asymmetry producing uneven spinal loading, excess body weight increasing compressive forces on the lumbar discs, low activity levels reducing the muscular support that offloads spinal compression, and prior trauma — including motor vehicle collision — that produces acute structural changes in a spine already compromised by existing curvature. See Refractory Spinal Pain After Car Accident Charlotte NC and Scoliosis After Car Accident Charlotte NC for how trauma intersects with existing scoliosis.
Scoliosis Progression Rates by Patient Category
| Patient Category | Typical Progression Rate | Key Risk Factors | Clinical Priority |
|---|---|---|---|
| Adolescent — Risser 0-1, active growth | Highly variable — can be rapid during growth spurt | Growth velocity, curve location, curve magnitude at diagnosis | Highest — intervention before significant growth is the best window |
| Adolescent — Risser 2-3, decelerating growth | Moderate — slowing with skeletal maturity | Remaining growth, thoracic vs lumbar location | High — bracing window may still be open |
| Adolescent — Risser 4-5, near or at maturity | Slow to stable | Curve magnitude at maturity, compliance with prior treatment | Moderate — consolidate gains and establish adult baseline |
| Adult — idiopathic, no active degeneration | 0.5 to 1 degree per year | Curve magnitude, activity level, posture | Moderate — cumulative over years |
| Adult — active degenerative changes | Up to 4 degrees per year | Disc height loss, facet arthropathy, excess load | High — degenerative scoliosis is almost universally progressive and painful |
| Geriatric — post-trauma or prior surgery | Variable — often accelerated | Hardware, altered biomechanics, bone density | High — see Geriatric Car Accident Injury Charlotte NC |
The Clinical Problem With Watch and Wait
The watch-and-wait recommendation for mild scoliosis in growing patients is not a neutral clinical decision. It is an active choice to allow the condition to evolve without intervention during the period when intervention is most likely to produce meaningful structural change. The reasoning behind it — that many mild curves do not progress significantly — is accurate at a population level. At the individual patient level, it is clinically inadequate without knowing that specific patient's Risser stage, growth velocity, curve location, and family history.
A Risser 0 patient with a 20-degree thoracic curve and a family history of scoliosis requiring surgery is not the same risk profile as a Risser 3 patient with a 20-degree lumbar curve and no family history. Applying the same watch-and-wait recommendation to both patients because they share the same Cobb angle measurement is not evidence-based risk stratification. It is a shortcut that occasionally works and occasionally results in a patient reaching the surgical threshold during an interval that could have been used for non-surgical intervention.
The Research and Evidence page at Clear Life Scoliosis covers the published literature on non-surgical scoliosis outcomes. The CLEAR Institute protocol — used by Dr. Justin Dick at Clear Life Scoliosis Charlotte NC — is specifically designed for the growth window that watch-and-wait leaves unused.
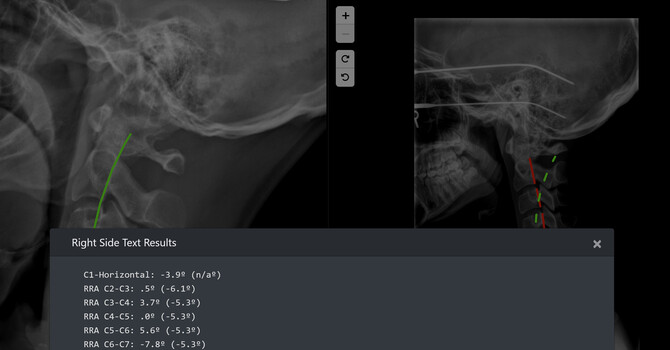
What the Cervical Spine Shows About Progression — Published Research at Clear Life
When to Intervene — The Timing Argument
For adolescent patients, the most mechanically favorable treatment window is prior to the first significant pubescent growth spurt — when the spine is still relatively flexible and the curve has not yet been amplified by rapid vertebral column lengthening. That window does not last indefinitely. Once significant growth has occurred and the curve has progressed, treatment can still produce improvement, but the magnitude of correction achievable and the treatment timeline both change.
For adult patients, the equivalent inflection point is the onset of degenerative changes. A 35-degree adult curve without active degeneration responds differently to conservative treatment than the same curve with active facet arthropathy and disc height loss. Intervening before the degenerative cycle becomes established is meaningfully easier than managing the condition once degeneration is driving progression.
Neither statement is an argument for unnecessary treatment. It is an argument for accurate progression risk assessment — knowing where a specific patient sits on the risk spectrum before deciding how urgently to intervene. See Treatment Options for the full framework at Clear Life Scoliosis Charlotte NC.
How Clear Life Charlotte Assesses Progression Risk
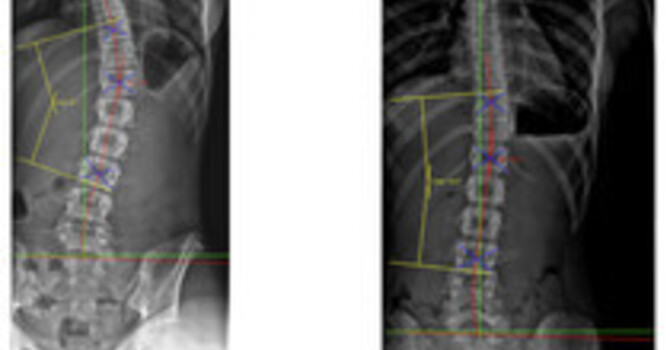
- Standing weight-bearing radiographs — Cobb angle measurement using PostureRay software, which has published inter- and intra-rater reliability data. Measurement variability up to 5 degrees is documented in the literature — knowing that variability exists and using a reliable measurement system matters for detecting real progression versus measurement artifact.
- Risser stage determination — from the AP standing radiograph at every initial evaluation for adolescent patients.
- Cervical radiographic evaluation including stress radiography — based on the published finding that abnormal C3-C4 segmental motion appears in over 70% of structural spinal injury patients. Not standard elsewhere. Standard at Clear Life.
- Curve flexibility assessment — lateral bending films where clinically indicated to determine the structural versus functional component of the curve.
- Serial measurement at defined intervals — progression is defined by change in Cobb angle over time. A single measurement establishes a baseline. Documented change over an interval establishes progression. The interval is calibrated to the patient's Risser stage and growth velocity, not set administratively.
Dr. Justin M. Dick, DC at Clear Life Scoliosis Charlotte NC holds CNMT and ARRT(N)(CT) dual imaging credentials — the only chiropractor in Charlotte with this combination — which directly informs how radiographic studies are acquired, measured, and interpreted. See Radiographic Imaging Credentials Charlotte NC for the full clinical framework.
Frequently Asked Questions — Scoliosis Progression Rate Charlotte NC
How fast does scoliosis progress in adolescents in Charlotte?
Adolescent scoliosis progression rate depends on Risser stage, growth velocity, and curve location — not curve magnitude alone. A Risser 0 patient during an active pubescent growth spurt can progress several degrees in a matter of weeks. Watch-and-wait monitoring at six-month intervals during this period can allow significant progression in the interim. Dr. Justin M. Dick, DC at Clear Life Scoliosis and Chiropractic Center — 8814 Rachel Freeman Way Suite 103, Charlotte NC 28278 — evaluates progression risk specifically before designing a treatment plan. No referral required. Call 980-368-0766.
Does scoliosis continue to progress in adults?
Yes. The assumption that scoliosis stabilizes at skeletal maturity is not supported by longitudinal data. Adult idiopathic scoliosis progresses at approximately 0.5 to 1 degree per year without intervention. When degenerative changes are active, progression can reach 4 degrees per year. Dr. Justin Dick at Clear Life Scoliosis Charlotte NC evaluates adult scoliosis patients for degenerative status as part of the standard assessment. Call 980-368-0766.
What is the Risser sign and why does it matter for scoliosis treatment in Charlotte?
The Risser sign is the degree of ossification of the iliac apophysis visible on a standing AP radiograph, graded 0 through 5. It is the most clinically useful marker of remaining skeletal growth. A Risser 0 patient has significant remaining growth and high progression risk. A Risser 5 patient has reached skeletal maturity. The Risser stage is one of the first determinations made in every adolescent scoliosis evaluation at Clear Life Scoliosis Charlotte NC. Call 980-368-0766.
How fast does degenerative scoliosis progress?
Degenerative scoliosis — driven by asymmetric disc height loss and facet joint arthropathy — can progress at up to 4 degrees per year once the degenerative cycle is established. Almost all cases of degenerative scoliosis are progressive and painful. A patient at 35 degrees with active degeneration can reach the surgical threshold of 50 degrees within several years without intervention. Dr. Justin Dick at Clear Life Scoliosis Charlotte NC evaluates degeneration status at every adult scoliosis assessment. Call 980-368-0766.
What is the surgical threshold for scoliosis?
The conventional surgical threshold for adolescent scoliosis is 45 to 50 degrees Cobb angle, at which point the risk of continued progression and the functional consequences of the deformity are considered to outweigh surgical risks. For adult degenerative scoliosis, the threshold is less well-defined and depends more on symptom burden and functional limitation than on Cobb angle alone. The goal of non-surgical treatment at Clear Life Scoliosis Charlotte NC is to prevent curves from reaching surgical threshold. Call 980-368-0766.
Can scoliosis progression be stopped without surgery in Charlotte?
Yes — in a meaningful proportion of patients when treatment is started at an appropriate time in the progression curve. The CLEAR Institute protocol used by Dr. Justin Dick at Clear Life Scoliosis Charlotte NC combines scoliosis-specific corrective exercise, spinal weighting, and custom bracing with serial radiographic monitoring. Published case series document Cobb angle stabilization and reduction at various severity levels. No treatment outcome can be guaranteed — but the evidence base for non-surgical intervention is strongest when treatment is started before significant progression has occurred. Call 980-368-0766.
Does Clear Life treat scoliosis patients from outside Charlotte NC?
Yes. Clear Life Scoliosis and Chiropractic Center provides scoliosis evaluation and treatment for patients from Charlotte, Huntersville, Ballantyne, Matthews, Concord, Mooresville, Rock Hill SC, and Fort Mill SC. Intensive treatment programs are available for out-of-area patients. No referral required. Call 980-368-0766.
Service Area
Clear Life Scoliosis and Chiropractic Center provides scoliosis evaluation and treatment — including Risser stage assessment, progression risk profiling, cervical radiographic evaluation, and CLEAR Institute protocol — for patients from Charlotte, Huntersville, Ballantyne, Matthews, Concord, Mooresville, Rock Hill SC, and Fort Mill SC. No referral required.
Assess Your Scoliosis Progression Risk at Clear Life Charlotte
Dr. Justin M. Dick, DC — CLEAR Fellow, CLEAR Board of Directors, CNMT, ARRT(N)(CT), multiple PubMed-indexed publications. Risser stage determination, cervical radiographic evaluation, serial Cobb angle measurement using PostureRay. No referral required. Cash-based practice.
Charlotte, NC 28278
980-368-0766 | office@clearlifescoliosis.com
Book Online at JaneApp
Justin Dick
Contact Me