Persistent spinal pain following motor vehicle collision (MVC) presents a particular challenge in older adults, especially in those with a history of lumbar surgery. Post-surgical alterations in spinal biomechanics, reduced tissue adaptability, and age-related degenerative change often complicate recovery. In such patients, clinical management frequently emphasizes pharmacologic symptom control or interventional escalation despite limited evidence of durable functional improvement in geriatric populations. Detailed case reports describing successful non-invasive structural rehabilitation in this demographic remain relatively uncommon.
In February 2026, Dick published a case report in Cureus describing the clinical course of a 66-year-old female who developed refractory lumbar pain following an MVC (Dick, 2026). The patient had a history of lumbar laminectomy, lumbar fusion (2022), cervical fusions (2006, 2009), and mild thoracic scoliosis. After the collision, she reported severe low back pain radiating into the lower extremity, persistent headache, and significant functional limitation. Standard medical management, including pharmacologic treatment and physical therapy, failed to produce meaningful improvement.
At presentation, the patient required a cane for ambulation and reported pain rated 8/10. Neurological examination demonstrated diffuse left-sided dermatomal sensory abnormalities spanning C5–T1 and L1–S1 distributions, with associated motor weakness graded 3/5 across multiple myotomes. The Functional Rating Index (FRI), a validated composite disability measure integrating elements of the Oswestry and Neck Disability Index, was 22/40, indicating substantial functional impairment.
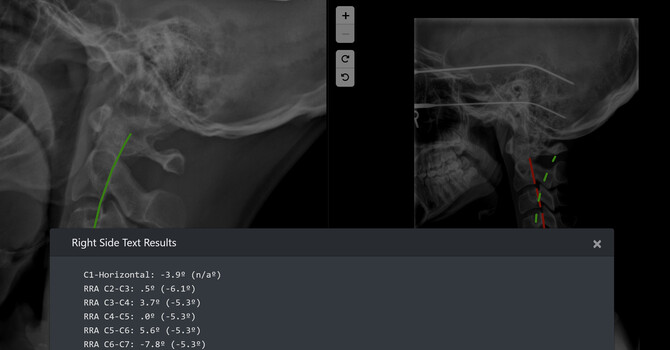
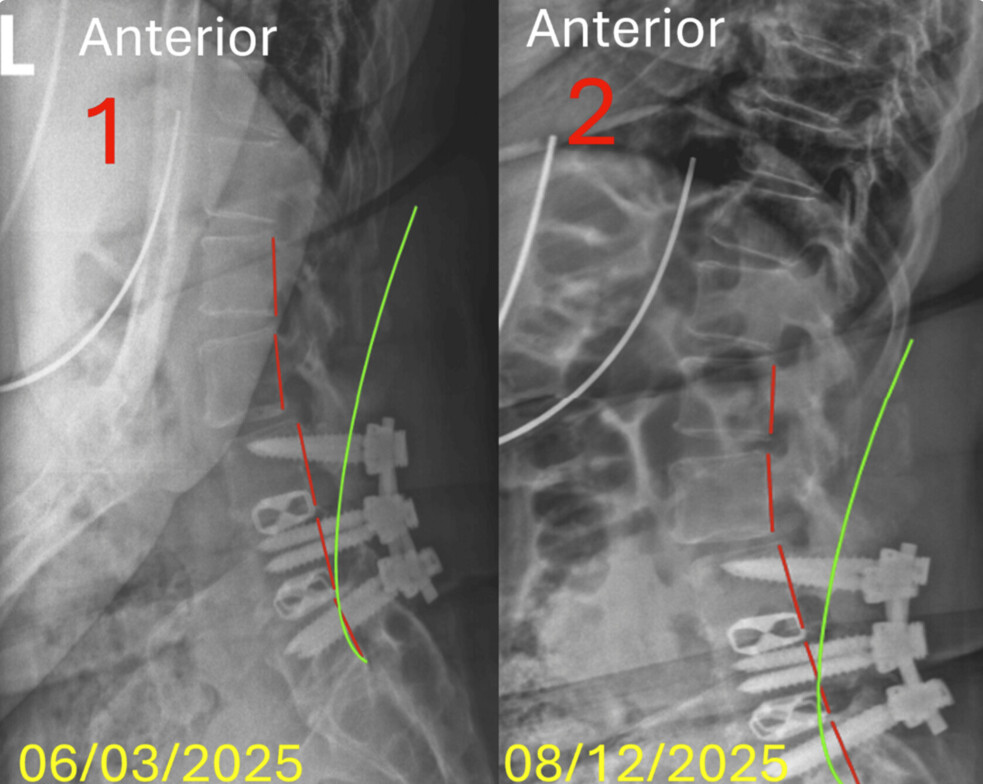
Radiographic assessment revealed decreased lumbar lordosis, anterior thoracic translation, persistent lateral thoracolumbar translation, and post-surgical degenerative changes. Cervical imaging similarly demonstrated reduced lordosis and anterior head translation. Structural alignment was quantified using the Absolute Rotation Angle (ARA) and translational metrics, allowing objective pre- and post-treatment comparison.
The patient underwent a 10-week multimodal conservative structural rehabilitation program totaling 23 visits. Interventions included pulsed electromagnetic field (PEMF) therapy, extracorporeal shockwave therapy (ESWT), and structural spinal rehabilitation derived from CLEAR Institute protocols. Treatment sessions followed a structured sequence emphasizing mobility preparation (“mix”), corrective mechanical intervention (“fix”), and neuromuscular stabilization (“set”). PEMF was applied at each visit to modulate inflammatory signaling and promote cellular repair. ESWT was administered weekly to the lumbar region for mechanical stimulation and nociceptive modulation. Structural correction targeted postural alignment and load distribution through individualized exercises and manual interventions.
At re-examination, conducted at least 24 hours after the final treatment session to reduce residual treatment effects, the patient demonstrated meaningful improvement. She no longer required assistive ambulation and reported complete resolution of radiating lumbar symptoms. Prescription analgesics were discontinued. FRI scores decreased from 22 to 11, reflecting a 50% improvement in disability. Neurological examination normalized, with resolution of prior dermatomal and myotomal deficits.
Radiographic measures demonstrated objective changes. Cervical lordosis improved from −20.4° to −23.2° (13.7% change), and anterior head translation decreased by 7%. Lumbar sagittal alignment demonstrated a reduction in anterior L1–S1 translation from 44.7 mm to 30.0 mm (32.9% improvement), with measurable modification of lordotic parameters. Although some values remained outside normative targets, directional improvement paralleled clinical resolution.
The case supports an emerging biomechanical framework in which persistent post-traumatic pain is not solely attributable to irreversible degenerative or surgical change. Instead, altered load distribution, sagittal misalignment, and neuromuscular dysregulation may represent modifiable contributors. In surgically altered spines, adjacent segment loading and compensatory mechanics can be amplified following acceleration–deceleration trauma. Addressing these structural variables through multimodal conservative intervention may interrupt pain perpetuation pathways, including nociceptive amplification and potential central sensitization.
Existing literature supports individual components of the protocol. PEMF has demonstrated anti-inflammatory and analgesic effects in chronic low back pain populations. ESWT has been shown to stimulate neoangiogenesis and modulate nociceptor activity. Structural rehabilitation approaches have documented alignment and functional improvements in selected spinal deformity cohorts. However, geriatric post-surgical MVC patients are often excluded from controlled trials, limiting the generalizability of available evidence. This case contributes descriptive data within that gap.
Interpretive caution is necessary. As a single case report, causal inference cannot be established. The relative contribution of each intervention cannot be isolated. Subject-specific variables, compliance, and non-specific treatment effects may have influenced outcomes. Nonetheless, the convergence of subjective improvement, neurological normalization, functional gain, and objective radiographic change strengthens the descriptive value of the observation.
Persistent lumbar pain in older adults carries consequences extending beyond symptom severity, including reduced mobility, increased fall risk, medication dependence, and decreased quality of life. In patients with prior lumbar surgery, such pain is frequently attributed to irreversible pathology, potentially narrowing therapeutic exploration. This case illustrates that conservative structural rehabilitation may represent a viable non-invasive pathway even in complex geriatric presentations.
Further research, including controlled comparative trials, is required to clarify efficacy, isolate treatment variables, and determine long-term durability. Until such data are available, detailed case reports remain valuable for hypothesis generation and clinical insight.
Reference
Dick, J. M. (2026). Refractory lumbar pain following motor vehicle collision in a geriatric patient with prior lumbar surgery: Clinical resolution after multimodal conservative spinal structural rehabilitation. Cureus, 18(2), e103540. https://doi.org/10.7759/cureus.103540
DOI:10.7759/cureus.103540.
Indexed in PubMed Central (PMCID:PMC12906243).
Clear Life Scoliosis and Chiropractic Center, Charlotte, North Carolina, USA
Clear Life Scoliosis and Chiropractic Center
specializes in finding and fixing the real cause of your discomfort. From advanced scoliosis treatment to personal injury recovery and preventive wellness care, we help Charlotte area residents reclaim their active lives. Call today and start your path to better movement, comfort, and control.
Justin Dick
Contact Me