It is common to see patients who were told after a car crash that they “should feel better in a few weeks.” A significant portion of them do not. That mismatch between expectation and reality is well documented in the biomechanics literature on whiplash-associated disorder (WAD), including work showing chronicity rates exceeding one-third of injured patients. This aligns closely with what we see locally in practice: symptoms often persist not because care was delayed out of negligence, but because the underlying injury was misunderstood. In clinical practice around Charlotte and the surrounding communities—Pineville, Tega Cay, Fort Mill, Berewick, we gert to the root cause of the problem.
One of the central challenges with whiplash injuries is that they often do not present with obvious structural damage on standard X-ray or MRI imaging. This has led to the mistaken assumption—frequently echoed by insurance carriers—that symptoms must therefore be muscular or self-limiting. However, decades of biomechanical research demonstrate that whiplash is primarily a soft tissue injury involving ligaments, joint capsules, and disc structures, particularly in the upper and mid-cervical spine. Muscles are rarely the primary pain generator, and that distinction matters when determining both prognosis and treatment.
The mechanics of a rear-impact collision explain why. Whiplash occurs in a sequence of rapid events measured in milliseconds. In the initial phase, the cervical spine undergoes a flexural deformation with an immediate reduction or loss of normal cervical lordosis. Within the first 50 milliseconds, both the upper and lower cervical segments experience flexion moments, while shear forces begin transmitting upward through the spine. Shortly thereafter, the spine transitions into a characteristic S-shaped curve, where the lower cervical vertebrae move into extension while the upper segments remain in relative flexion. This creates opposing forces across motion segments, particularly at C5–C6, which consistently shows the earliest and greatest rotational stress. In the final phase, the entire cervical spine is driven into extension under tensile and shear loads.
From a clinical standpoint, these forces disproportionately stress the facet joint capsules, intervertebral discs, and upper cervical ligaments. Studies repeatedly identify facet capsule injury as a primary source of chronic neck pain following whiplash. These injuries may include ligament tears, cartilage damage, hemarthrosis, and even microfractures—none of which are reliably visible on routine imaging. Disc injuries, including annular fiber tears and endplate avulsions, as well as injuries to major stabilizing ligaments like the anterior longitudinal ligament, are also common findings in experimental and post-mortem studies.
This helps explain why symptoms can worsen over time rather than improve. Many patients experience a brief symptom-free or low-pain interval before pain, stiffness, headaches, dizziness, or cognitive complaints emerge more fully. In the Charlotte region, where long commutes on I-77 and I-485 are common, we frequently see delayed symptom escalation as patients resume normal driving, work, and caregiving demands. Epidemiological data show that while roughly two-thirds of patients recover within three months, a substantial minority develop persistent symptoms lasting longer than six months—often labeled as late whiplash syndrome.
Muscle strain is often cited as the presumed injury, but this explanation does not hold up biomechanically or clinically. During a rear-impact collision, anterior neck muscles such as the sternocleidomastoid are theoretically stretched, yet most patients report posterior neck pain. Experimental data also show that muscle tissue generally fails only under forces far exceeding those seen in whiplash, particularly when compared to the vulnerability of ligamentous structures. Additionally, during the critical moments of impact, the large posterior extensor muscles are under compression and unlikely to contract in a way that would generate acute injury. This further supports the conclusion that muscle strain is not the primary driver of ongoing symptoms.
Shear forces play a particularly important role. As the seatback accelerates the torso forward and the head lags behind due to inertia, the thoracic spine straightens and transmits compressive forces upward into the cervical spine. This compression, combined with anterior shear at each vertebral level, causes adjacent vertebrae to slide relative to one another. The facet joint capsules are stretched, pinched, and compressed—especially in their posterior regions—activating pain-sensitive structures and setting the stage for inflammation and chronic instability.
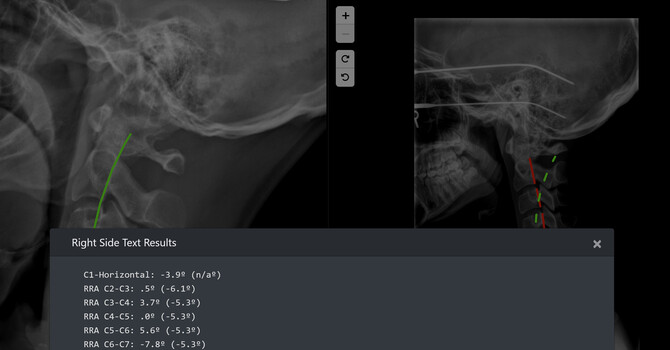
Understanding these mechanisms is not academic—it directly informs how we document injuries, educate patients, and design care plans. In my work at Clear Life Scoliosis in the Charlotte, North Carolina area, careful attention to cervical alignment, segmental motion, and ligament integrity is essential, particularly in patients who present weeks or months after a collision. When these injuries are recognized early and managed appropriately, outcomes improve. When they are dismissed as “just muscle strain,” chronic pain becomes far more likely.
Whiplash-associated disorder is not a mysterious or exaggerated condition. It is a well-characterized biomechanical injury with predictable patterns and known pain generators. Recognizing that reality allows clinicians to provide more accurate diagnoses, set realistic expectations, and offer care that addresses the true source of injury rather than its superficial symptoms.
Clear Life Scoliosis and Chiropractic Center, Research focus in finding and fixing the real cause of your discomfort. From advanced scoliosis treatment to personal injury recovery, we help Charlotte area residents reclaim their active lives. Call today and start your path to better movement, comfort, and control.
Biomechanics of whiplash injury - PubMed
Chinese Journal of Traumatology 2009; 12(5):305-314 . 305 . DOI: 10.3760/cma.j.issn.1008-1275.2009.05.011 Daping Hospital, Third Military Medical University, Chongqing 400042, China Chin J Traumatol 2009; 12(5):305-314 Biomechanics of whiplash injury CHEN Hai-bin 陈海
Justin Dick
Contact Me