Swimming gets recommended for scoliosis constantly. Parents ask about it at every initial evaluation. The recommendation usually comes from a pediatrician, a physical therapist, or a well-meaning relative who heard that swimming is good for the spine. Sometimes it comes from a quick internet search. The answer is not as simple as the recommendation makes it sound.
Swimming does specific things well. It works muscles symmetrically. It reduces gravitational compressive load on the spine. It maintains cardiovascular fitness and flexibility. These are real benefits — for a person with scoliosis and for a person without scoliosis. What swimming does not do is treat the structural three-dimensional deformity that scoliosis is. That distinction matters enormously for a family deciding how to manage their child's curve.
The clinical answer in one paragraph:
Recreational swimming is appropriate and beneficial for most patients with scoliosis as general conditioning. It should not replace scoliosis-specific treatment. Competitive swimming — 4 to 6 hours per day in the pool — requires careful clinical evaluation because of the prolonged cervical hyperextension and asymmetric loading that specific strokes produce. And backstroke, commonly recommended as "scoliosis-safe," introduces its own cervical mechanics issues that are directly relevant to Dr. Dick's published research findings on cervical dysfunction in scoliosis patients.
Why Swimming Was Once Thought to Treat Scoliosis
The gravity hypothesis drove the original enthusiasm for swimming as a scoliosis treatment. The thinking went like this: gravity loads the spine compressively in an upright position and contributes to curve progression; swimming eliminates gravitational load; therefore swimming reduces curve progression.
The hypothesis was clinically plausible and turned out to be wrong — or at least incomplete. The primary driver of scoliosis progression in adolescents is not gravitational loading. It is skeletal growth. The lengthening motion the spine experiences during growth is what triggers the pathomechanical cascade that increases the Cobb angle. A child with a 25-degree curve at Risser 0 who swims daily is still growing. Their curve will progress during that growth regardless of how many hours they spend in the pool.
The gravity hypothesis also failed to account for the three-dimensional nature of scoliosis. A scoliotic curve is not simply a side-to-side bend that compressive loading makes worse. It is a coupled deformity — coronal curve, axial rotation, and sagittal change occurring simultaneously. Reducing gravitational compression addresses one dimension of a three-dimensional problem. The rotational and sagittal components are unaffected by buoyancy.
What Swimming Actually Does for the Scoliotic Spine
The Benefits — What Is Real and Why
Symmetric muscle activation. Most sports and activities involve asymmetric loading — one side of the body working harder than the other. Swimming, particularly freestyle and breaststroke, activates paraspinal and core musculature more symmetrically than most land-based exercise. For a scoliosis patient whose curve produces habitual asymmetric loading, symmetric muscle activation is genuinely useful. It does not correct the curve but it can reduce the secondary muscle imbalance that compounds the structural deformity.
Spinal decompression. Horizontal body position in water reduces axial compressive loading on the intervertebral discs and facet joints. For adult scoliosis patients where degenerative changes are producing pain through asymmetric compressive loading, swimming provides a pain-relieving activity that does not aggravate the mechanical pain pattern. This is a real clinical benefit — not a treatment, but a genuine quality-of-life improvement.
Cardiovascular fitness and flexibility maintenance. Scoliosis patients who avoid activity because of discomfort or body image concerns are at risk for deconditioning that compounds their functional limitations. Swimming is a non-impact activity that maintains cardiovascular fitness and hamstring, hip flexor, and thoracic flexibility without the joint loading of running or court sports. For adolescent patients who are discouraged from contact sports during active bracing — swimming is often the right activity recommendation.
Pain management. The combination of buoyancy, warm water, and symmetric muscle activation produces meaningful pain relief for scoliosis patients with pain-generating curves. This is a quality-of-life benefit that is clinically significant even when it produces no change in Cobb angle.
The Limitations — What Swimming Cannot Do
Swimming cannot produce ligament remodeling. The mechanism that produces structural Cobb angle reduction in scoliosis is sustained corrective loading of spinal ligaments in the mirror image of the deformity — a mechanism that requires directional force applied with specificity to the curve pattern. Buoyancy eliminates the gravitational load but does not replace it with corrective directional load. The water does not know your child's curve type.
Swimming cannot correct axial rotation. The rotational component of scoliosis — the vertebral rotation that produces the rib prominence visible on Adam's forward bend test — is the most clinically significant and the most difficult to treat. No swimming stroke addresses vertebral rotation specifically. The Schroth Method and the CLEAR Institute protocol both address rotation through curve-specific positioning and loading that cannot be replicated in a pool.
Swimming cannot replace curve-specific exercise. The scoliosis-specific exercise systems with published evidence — SEAS and Schroth — work through active self-correction in positions specific to each patient's curve pattern. The muscle activation patterns in these systems are fundamentally different from the symmetric activation swimming produces. Swimming can be done in addition to these programs. It cannot substitute for them.
The Competitive Swimming Problem — Why Hours in the Pool Change the Equation
Recreational swimming — 30 to 60 minutes several times per week — is a different clinical question from competitive swimming at 4 to 6 hours per day. The difference matters for three specific reasons.
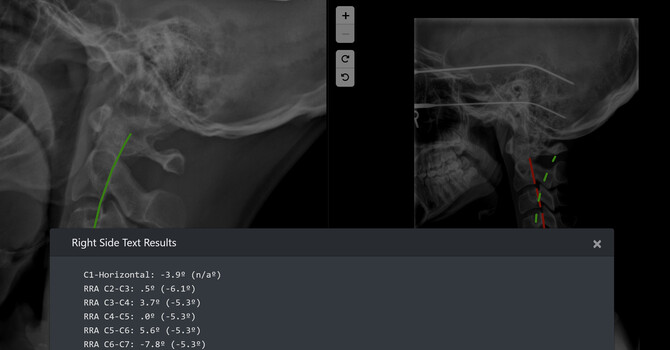
Cervical hyperextension in freestyle. The most common competitive stroke — freestyle — requires prolonged cervical hyperextension to keep the face out of the water during breathing. A swimmer who swims 5,000 meters per practice is spending significant cumulative time with the cervical spine in sustained hyperextension. For a scoliosis patient whose cervical spine is already mechanically compromised — Dr. Dick's published research found cervical lordosis loss in 100% of scoliosis patients — sustained hyperextension loads an already-dysfunctional cervical structure in ways that can produce pain, headache, and neurological symptoms.
Asymmetric breathing patterns. Competitive swimmers typically breathe to one preferred side during freestyle. Consistent one-sided breathing rotation produces cumulative asymmetric loading through the cervical and upper thoracic spine. For a scoliosis patient with a right thoracic curve who consistently rotates right to breathe, that loading pattern reinforces the asymmetry of the existing deformity rather than counteracting it.
Volume of unloaded time. A competitive swimmer who is in the pool for 5 hours per day spends 5 hours in a horizontal, buoyant, decompressed position. The proprioceptive feedback the spine uses to maintain upright posture is eliminated for that duration. Some published data suggests that prolonged elimination of gravitational feedback — the same feedback that scoliosis patients are already processing abnormally through a compromised righting reflex mechanism — may have negative consequences for postural control that extend beyond the pool session.
The backstroke question:
Backstroke is frequently recommended as the most "scoliosis-friendly" competitive stroke because it involves a supine position and bilateral symmetric arm movement. This recommendation is clinically reasonable but incomplete. Backstroke still requires bilateral cervical rotation during the stroke cycle and sustained cervical positioning that loads the upper cervical structures. For a scoliosis patient with documented C3-C4 segmental instability — a finding present in over 70% of Dr. Dick's scoliosis research cohort — the cervical loading of competitive backstroke is not clinically neutral. A formal evaluation of cervical mechanics is the appropriate basis for stroke selection in a competitive swimmer with scoliosis, not a generic recommendation.
The Cervical Connection — Why This Matters More Than Most Providers Realize
Dr. Justin Dick's published research on cervical mechanics in scoliosis patients — PMID 41018459, recognized at IRAPS 2026 at Sherman College of Chiropractic — found that 100% of adolescent scoliosis patients had lost normal cervical lordosis and over 70% had abnormal segmental translation at C3-C4.
This finding is directly relevant to the swimming question in a way that most scoliosis guidance does not address. The righting reflex — the neurological system that keeps the eyes level with the horizon — operates through the cervical spine. When cervical mechanics are abnormal, the righting reflex receives distorted proprioceptive input and the global spinal compensation pattern is affected. Swimming strokes that repeatedly load an already-dysfunctional cervical spine in sustained extension or rotation are not clinically neutral for this patient population.
This is not an argument against swimming for scoliosis patients. It is an argument for evaluating cervical mechanics before making a swimming recommendation — something that no other scoliosis practice in Charlotte does as part of routine evaluation and something that Dr. Dick's published research has established as clinically necessary.
How to Think About Swimming If Your Child Has Scoliosis
The clinical framework for evaluating swimming in a scoliosis patient involves four questions:
- What is the curve size and Risser stage? A 12-year-old at Risser 0 with a 25-degree curve is in a fundamentally different risk category than a 17-year-old at Risser 4 with the same curve. The former needs active treatment. The latter may appropriately focus on maintenance. Swimming recommendation changes based on this risk stratification.
- What are the cervical mechanics? A scoliosis patient with documented C3-C4 instability who wants to compete in freestyle needs a cervical-aware stroke modification recommendation — not a generic clearance. This requires cervical radiographic evaluation that the evaluation at Clear Life provides.
- What is the treatment plan? Swimming during active CLEAR protocol treatment is appropriate and often recommended. Swimming as a substitute for a treatment plan is not appropriate for a curve that is progressing or at risk of progressing.
- What are the training demands? Recreational swimming and competitive swimming are different clinical scenarios. A child who swims recreationally twice per week and a child who trains 20 hours per week at a competitive club require different clinical conversations.
Sports and Activities — A Clinical Framework for Scoliosis Patients
What Actually Treats Scoliosis — The Clinical Standard at Clear Life
Swimming, yoga, Pilates, and general exercise are appropriate components of a scoliosis patient's life. They are not treatment. The distinction matters because families who pursue general exercise in place of scoliosis-specific treatment lose the treatment window — the growth period during which structural correction is most achievable and the progression risk is highest.
The CLEAR Institute multimodal protocol at Clear Life Scoliosis addresses scoliosis as a three-dimensional structural problem — five components targeting the specific mechanisms of the deformity that no exercise program reaches:
- Whole body vibration — neurological priming for exercise and correction
- Scoliosis-specific exercise — curve-specific activation incorporating SEAS and Schroth principles, not generic core strengthening
- Mirror image adjustment — directionally specific adjustment opposite to the scoliotic deviation
- Mirror image traction — sustained corrective loading for ligament remodeling — the mechanism that produces Cobb angle reduction that exercise alone cannot replicate
- Cervical correction — addressing the cervical dysfunction that Dr. Dick's published research found in 100% of scoliosis patients
A patient who swims three times per week and completes the CLEAR protocol on treatment days is combining general fitness with structural treatment appropriately. A patient who swims three times per week instead of pursuing structural treatment is doing one thing when two things are needed.
Frequently Asked Questions — Scoliosis and Swimming
Is swimming good for scoliosis?
Recreational swimming is appropriate and beneficial for most scoliosis patients as a general conditioning activity. It works muscles symmetrically, reduces spinal compressive loading, maintains cardiovascular fitness, and provides pain relief. It does not produce Cobb angle reduction and does not replace scoliosis-specific structural treatment. Dr. Justin Dick at Clear Life Scoliosis and Chiropractic Center in Charlotte, NC — CLEAR Fellow, ISICO World Masters, multiple PubMed-indexed publications — evaluates and treats scoliosis. No referral required. Call 980-368-0766.
Can swimming make scoliosis worse?
Recreational swimming does not make scoliosis worse in most patients. Competitive swimming — at high volumes with prolonged cervical hyperextension in freestyle and asymmetric breathing patterns — warrants clinical evaluation before being cleared for patients with scoliosis, particularly those with documented cervical mechanics abnormalities. Dr. Dick's published research found abnormal cervical segmental motion in over 70% of scoliosis patients — a finding directly relevant to high-volume competitive swimming. Dr. Justin Dick at Clear Life Scoliosis Charlotte NC evaluates cervical mechanics as part of every scoliosis assessment. Call 980-368-0766.
Is backstroke the best swimming stroke for scoliosis?
Backstroke is often recommended as the most scoliosis-friendly competitive stroke because of its bilateral symmetric arm movement and supine position. This recommendation is reasonable but incomplete. Backstroke still involves cervical rotation during the stroke cycle and sustained cervical positioning. For scoliosis patients with documented C3-C4 cervical instability — present in over 70% of Dr. Dick's research cohort — stroke selection should be based on a cervical mechanics evaluation rather than a generic recommendation. Call Clear Life Scoliosis Charlotte NC at 980-368-0766.
Should my child stop swimming if they have scoliosis?
Recreational swimming does not need to stop for a child with scoliosis. Competitive swimming at high training volumes requires clinical evaluation — specifically of cervical mechanics and curve-specific loading during specific strokes. The more important clinical question is whether swimming is being used in place of scoliosis-specific structural treatment, because that treatment window — the growth period when structural correction is most achievable — is time-limited. Dr. Justin Dick at Clear Life Scoliosis Charlotte NC, 8814 Rachel Freeman Way Suite 103, provides this evaluation. No referral required. Call 980-368-0766.
What exercise is best for scoliosis?
Scoliosis-specific exercise — not general exercise — has the published evidence base for slowing progression and producing functional improvement in scoliosis. SEAS (Scientific Exercise Approach to Scoliosis) and the Schroth Method are the two most evidence-supported scoliosis-specific exercise systems. The CLEAR Institute protocol integrates scoliosis-specific exercise as one of five components. General exercise — swimming, yoga, Pilates, walking — is appropriate as an adjunct. It is not a substitute for scoliosis-specific treatment. Dr. Justin Dick at Clear Life Scoliosis Charlotte NC provides scoliosis-specific exercise as part of the CLEAR protocol. Call 980-368-0766.
Can adults with scoliosis swim?
Yes. Swimming is particularly appropriate for adult scoliosis patients where the primary goals are pain management, functional preservation, and cardiovascular fitness. The decompressive effect of buoyancy reduces asymmetric facet and disc loading that drives pain in adult scoliosis. Adults who swim regularly as part of a broader management program that includes structural correction, bracing for offloading, and scoliosis-specific exercise tend to have better functional outcomes than adults who pursue any single activity in isolation. Dr. Justin Dick at Clear Life Scoliosis Charlotte NC treats adult scoliosis. Call 980-368-0766.
Is swimming a treatment for scoliosis?
No. Swimming is a general conditioning activity that produces real benefits for scoliosis patients — symmetric muscle activation, spinal decompression, pain relief, and cardiovascular fitness. It does not produce the ligament remodeling that reduces Cobb angle, does not address vertebral rotation, and does not deliver the curve-specific correction that scoliosis-specific exercise systems and structural correction produce. The distinction between swimming as a beneficial adjunct and swimming as a treatment is the most important clinical point for any family managing a scoliosis diagnosis. Dr. Justin Dick at Clear Life Scoliosis Charlotte NC treats scoliosis with the CLEAR Institute protocol. Call 980-368-0766.
Evaluate Your Child's Scoliosis at Clear Life — Charlotte NC
Whether your child swims recreationally, competes at a club level, or has been told to swim for their scoliosis — a specialist evaluation at Clear Life includes cervical mechanics assessment, Cobb angle measurement, Risser staging, and a direct clinical conversation about what their curve needs and what activity is appropriate during treatment.
No referral required. Cash-based practice.
→ Book Your Evaluation | Call 980-368-0766
Clear Life Scoliosis and Chiropractic Center · 8814 Rachel Freeman Way, Suite 103 · Charlotte, NC 28278
Justin Dick
Contact Me